Dialysis Transportation: An NEMT Provider's Guide
End-Stage Renal Disease (ESRD) patients who receive in-center hemodialysis need a round trip to a dialysis center three times a week, 52 weeks a year. That works out to 156 scheduled rides per patient, on a fixed calendar, with no option to skip. No other trip type in NEMT has that structure.
Contents:
- Why Dialysis Is the Anchor Contract in NEMT
- What Dialysis Requires That Other Trips Don't
- How the Money Flows to Providers
- Where Margins Get Made or Lost
- How to Get Into Dialysis Contracts
- Final Thoughts
Why Dialysis Is the Anchor Contract in NEMT
About 433,000 people in the US receive in-center hemodialysis as of March 2025, according to the National Forum of ESRD Networks. Each one goes three times a week, most on a Monday/Wednesday/Friday or Tuesday/Thursday/Saturday schedule. The pickup address doesn't change. The destination doesn't change. The schedule doesn't change. You can plan a week out with near-perfect confidence about what you're dispatching.
32.6 NEMT ride-days per year for ESRD patients vs. 0.4 for the general Medicaid population — roughly 80 times the average rate. (MACPAC, 2021)
Research published in the American Journal of Kidney Diseases found that transportation problems account for 81% of missed dialysis treatments, and missing a session raises a patient's adjusted mortality risk by 68%. People don't skip dialysis because they feel fine that day. They miss it because something went wrong with the ride. That makes your on-time performance a direct factor in patient outcomes, and the frame that gets the attention of facility staff when you're trying to win their referrals.
What Dialysis Requires That Other Trips Don't
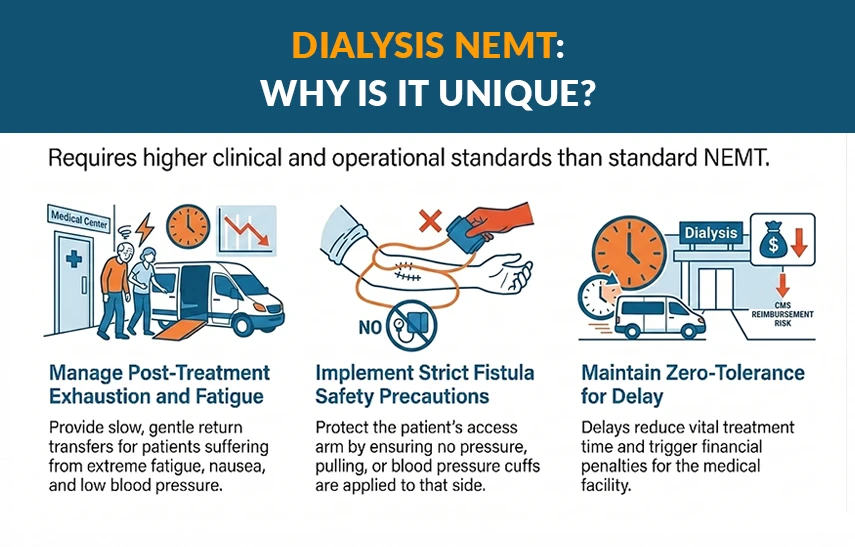
A standard NEMT trip involves picking someone up and getting them to an appointment. Dialysis adds three things that don't exist on most other runs.
- Post-treatment patient state. By the time a patient finishes a four-hour session, they're physically drained. Intradialytic hypotension, a significant drop in blood pressure during treatment, affects between 5 and 30% of hemodialysis sessions according to KDOQI and European Best Practice Guidelines. Add fatigue, muscle cramping, and occasional nausea. Drivers need to expect slower transfers on the return and allow time to stabilize before moving.
- Fistula precautions. Most in-center HD patients have an arteriovenous fistula or graft, the access point used during dialysis. The KDOQI 2019 Vascular Access Guidelines set the standard: no blood pressure cuffs, no compression, no venipuncture on the access arm. Drivers just need to know which arm to avoid and document it. This belongs in onboarding and in the vehicle checklist.
- Punctuality influences healthcare outcomes. A late arrival doesn't just generate a complaint. When a patient misses part of a session, their dialysis adequacy drops. CMS tracks this under a metric called Kt/V as part of the ESRD Quality Incentive Program. Facilities that fall short of QIP thresholds can lose up to 2% of their Medicare reimbursement for an entire payment year. On-time performance is what you sell to facility social workers when you want their patient referrals. It's not a soft differentiator.
Most dialysis patients are older and many have limited mobility. Your NEMT training program needs to cover both passenger handling and fistula precautions. Wheelchair safety standards apply here from day one.
How the Money Flows to Providers
Medicaid pays for routine dialysis transportation. Under 42 CFR § 431.53, every state Medicaid plan is required to ensure transportation to covered services. Because dialysis is life-sustaining, it qualifies automatically. In most states, the money flows through a capitated broker before it reaches the provider. The broker, typically Modivcare, MTM, or a state-specific equivalent, manages scheduling, handles credentialing, and sets the rates. If you're not yet enrolled, start with how to become a Medicaid transportation provider.
Here's how the three main payer types break down:
- Medicaid: Covers routine dialysis rides. Flows through a state-managed or broker-administered program. This is your primary and most reliable revenue source.
- Medicare Part B: Covers ground ambulance transport to dialysis only when the patient's condition makes other transport medically contraindicated, per CMS Medicare Benefit Policy Manual Chapter 10. A patient who walks or uses a wheelchair doesn't qualify. Don't bid Medicare ambulance work you're not certified to perform.
- Medicare Advantage: Some plans offer supplemental transportation benefits, but the coverage is shrinking. In 2025, 30% of individual MA plans included a medical transportation benefit. By 2026, that dropped to 24% (KFF). Among Special Needs Plans, which serve dual-eligible patients most likely to need dialysis transport, the share fell from 81% to 67% in the same period. Don't build a dialysis program around MA volume.
About 45% of dialysis patients are dually eligible for Medicare and Medicaid, according to the American Kidney Fund. These patients rely on Medicaid for transport even though Medicare is their primary health insurer. See also which insurance providers pay for NEMT.
Where Margins Get Made or Lost
Published state Medicaid NEMT rates give a concrete floor to work from. In Colorado, as of the 2025-2026 Health First Colorado billing manual, ambulatory and wheelchair-van transport pays $12.40 per trip base plus $2.80 per loaded mile. The structure is consistent across most states: base fee plus loaded mileage only. Deadhead miles are not compensated.
That uncompensated deadhead is where dialysis routes bleed. Morning pickups are residential addresses spread across your service area. Drops land at a small number of centers. The return leg reverses the pattern. If you're running both halves without filling the dead miles, the route loses money on every trip. There's a full breakdown of strategies for crushing deadhead miles that applies directly to dialysis route planning.
Route density fixes it. Cluster morning pickups by geography, batch ambulatory patients on shared runs, and sequence arrivals within the center's intake window. Multi-loading is the tactic that makes dialysis economics work. Wheelchair trips limit batching but still benefit from geographic grouping.
Brokers run capitated contracts, which means when your trip volume rises, the rate doesn't move with it. Modivcare's 2024 Form 10-K shows 80.9% of its NEMT revenue under capitated arrangements. If a single broker accounts for more than 40 to 50% of your dialysis revenue, that's a structural risk worth managing. For context on profitability at typical Medicaid rates, this post works through the math.
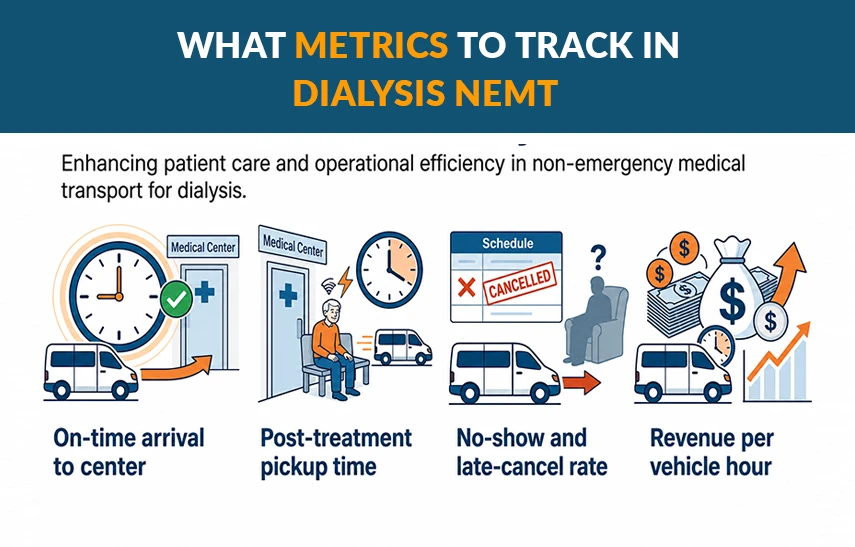
Four numbers tell you whether the program is working; track them with consistent reporting across your operation:
- On-time arrival to center: Aim above 95%. Late arrivals shorten treatment time and create QIP exposure for the facility.
- Post-treatment pickup time: Centers run on shift schedules. A late return holds the chair for the next patient.
- No-show and late-cancel rate: A study of 44 million US hemodialysis treatments published in the Journal of the American Society of Nephrology found that transportation problems account for about 0.9 missed sessions per patient per year — roughly 0.6% of all scheduled trips. That's the national floor. Target staying at or below 1%.
- Revenue per vehicle hour: The number that tells you whether your batching is working or whether deadhead is still eating the margin.
How to Get Into Dialysis Contracts
The US dialysis market is highly concentrated. A 2025 JAMA Health Forum study found DaVita and Fresenius together held 77% of US dialysis facilities by 2019, up from 59% in 2005. DaVita operated 2,657 US centers as of December 2024. Fresenius runs an estimated 2,600 to 2,800. Of the 7,556 total US facilities, independent and hospital-based centers account for roughly 10%. Dialysis transportation at scale runs through a handful of large chain relationships and the Medicaid brokers that serve them.
The broker path is faster. Credential with the Medicaid broker in your state, enter their provider network, and trip assignments start coming. Rates are preset and volume is broker-determined. See the guides for Modivcare and MTM for what each broker expects.
The facility relationship path holds better. Local DaVita and Fresenius clinic managers, social workers, and patient care technicians influence which providers their patients use for standing orders. Bring on-time data and a documented driver protocol to those conversations. For providers building their first contracts, how to get medical transportation contracts covers the groundwork.
Concentration risk cuts both ways. Winning a cluster of DaVita centers in a metro area is efficient. Losing it because DaVita shifted broker networks removes a large revenue block at once. Diversify before that becomes a problem.
Final Thoughts
Dialysis transportation is predictable in a way that almost nothing else in NEMT is. The schedule is fixed, the locations repeat, and the demand doesn't go away between seasons. Where providers lose the margin is in the recurring workflows: standing orders rescheduled by hand, routes built for single trips instead of clusters, and billing that falls behind the trip cycle. RouteGenie automates all three. Request a RouteGenie demo to see how it handles recurring dialysis operations.
About the author

Serhii Taborovskyi is the founder and author of the Automotive Territory YouTube Channel, with 300,000 subscribers and counting. He is an avid automotive enthusiast and a fan of any and all motorized vehicles. Serhii is a visiting author at RouteGenie, sharing his expertise for the benefit of the NEMT community.